 Overview Overviewhammertoes is a contracture (bending) of one or both joints of the second, third, fourth, or fifth (little) toes. This abnormal bending can put pressure on the toe when wearing shoes, causing problems to develop. Hammertoes usually start out as mild deformities and get progressively worse over time. In the earlier stages, hammer toes are flexible and the symptoms can often be managed with noninvasive measures. But if left untreated, hammer toes can become more rigid and will not respond to non-surgical treatment. Because of the progressive nature of hammertoes, they should receive early attention. Hammertoes never get better without some kind of intervention. Causes Hammer toe is often caused by wearing shoes that do not fit properly. If shoes are too small either in length or width, then the toes are Hammer toe held in a shortened position for long periods and the muscles eventually shorten and pull the toes into the bent position. Alternatively it can be caused by overactivity in the extensor digitorum dongus muscle (right) and a weakness in the counteracting muscle under the foot, such as flexor digitorum longus. Sometimes it can be a congenital condition, meaning it is present from birth. It is also more common in those with arthritis in the foot or diabetes.  Symptoms SymptomsHammer toe is often distinguished by a toe stuck in an upside-down ?V? position, and common symptoms include corns on the top of your toe joint. Pain at the top of a bent toe when you put on your shoes. Pain when moving a toe joint. Pain on the ball of your foot under the bent toe. Corns developing on the top of the toe joint. It is advisable to seek medical advice if your feet hurt on a regular basis. It is imperative to act fast and seek the care of a podiatrist or foot surgeon. By acting quickly, you can prevent your problem from getting worse. Diagnosis Some questions your doctor may ask of you include, when did you first begin having foot problems? How much pain are your feet or toes causing you? Where is the pain located? What, if anything, seems to improve your symptoms? What, if anything, appears to worsen your symptoms? What kind of shoes do you normally wear? Your doctor can diagnose hammertoe or mallet toe by examining your foot. Your doctor may also order X-rays to further evaluate the bones and joints of your feet and toes. Non Surgical Treatment Apply a commercial, nonmedicated hammertoe pad around the bony prominence of the hammertoe. This will decrease pressure on the area. Wear a shoe with a deep toe box. If the hammertoe becomes inflamed and painful, apply ice packs several times a day to reduce swelling. Avoid heels more than two inches tall. A loose-fitting pair of shoes can also help protect the foot while reducing pressure on the affected toe, making walking a little easier until a visit to your podiatrist can be arranged. It is important to remember that, while this treatment will make the hammertoe feel better, it does not cure the condition. A trip to the podiatric physician?s office will be necessary to repair the toe to allow for normal foot function. Avoid wearing shoes that are too tight or narrow. Children should have their shoes properly fitted on a regular basis, as their feet can often outgrow their shoes rapidly. See your podiatric physician if pain persists. Surgical Treatment Sometimes, if the deformity is severe enough or surgical modification is needed, the toe bones may be fused so that the toe does not bend. Buried wires are used to allow for the fusion to heal, and they remain in place after healing. Your skin is closed with fine sutures, which are typically removed seven to ten days after surgery. A dressing is used to help keep your toes in their new position. Dressings should not get wet or be removed. After surgery, your doctor may prescribe pain relievers, typically for the initial four to seven days. Most people heal completely within one month of surgery, with few complications, if any. Crutches or a cane may be needed to help you keep weight off your affected foot, depending on the procedure. Occasionally, patients receive a special post-op shoe or a walking boot that is to be worn during the healing process. Most people are able to shower normally after surgery, but must protect the dressing from getting wet. Many patients are allowed to resume driving within one week after the procedure, but care needs to be taken.
Overview
 A bunion is an enlargement at the base of the big toe caused by a misalignment of the joint. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position. of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as ?bunions?. Bunions are really only a symptom of faulty foot mechanics and are usually caused by the foot we inherit and inappropriate footwear use. As the big toe bends towards the others this lump becomes larger and the bunion can become painful - arthritis and stiffness can eventually develop. A bunion is an enlargement at the base of the big toe caused by a misalignment of the joint. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position. of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as ?bunions?. Bunions are really only a symptom of faulty foot mechanics and are usually caused by the foot we inherit and inappropriate footwear use. As the big toe bends towards the others this lump becomes larger and the bunion can become painful - arthritis and stiffness can eventually develop.Causes Although they may develop on the fifth (little) toe, bunions usually occur at the base of the big toe. Bunions are often caused by incorrect foot mechanics. The foot may flatten too much, forcing the toe joint to move beyond normal range. In some cases, joint damage caused by arhritis or an injury produces a bunion. And some people are simply born ith extra bone near a toe joint. If you're at risk for developing a bunion, wearing high-heeled or poorly fitting shoes make the problem worse. As new bone grows, the joint enlarges. This stretches the joint's outer covering. Force created by the stretching pushes the big toe toward the smaller ones. Eventually, the inside tendons tighten, pulling the big toe farther out of alignment. Symptoms Look for an angular, bony bump on the side of the foot at the base of the big toe. Sometimes hardened skin or a callus covers this bump. There's often swelling, redness, unusual tenderness, or pain at the base of the big toe and in the ball of the foot. Eventually, the area becomes shiny and warm to the touch. Seek medical advice if you have persistent pain when walking normally in otherwise comfortable, flat-soled shoes, you may be developing a bunion, bursitis, or a bone spur in your foot. Diagnosis Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly. Non Surgical Treatment You can buy orthotics over the counter from pharmacies, or they can be custom-made by a podiatrist to fit your feet. Whether you need to buy an over-the-counter orthotic or have one specially made will depend on your individual circumstances and the severity of your bunion. You can also use special bunion splints, worn over the top of your foot and your big toe to help straighten its alignment. Splints are available for both daytime and night-time use. However, there's little evidence that splints are effective. Toe spacers are also available, which can help reduce the pain caused by bunions. However, toe spacers or orthotics may be of limited use because they often compete with the bunion for the already limited space in the shoe. If your toe joint is painful and swollen, applying an ice pack to the affected area several times a day can help to relieve the pain and inflammation. Never apply ice directly to your skin. Wrap it in a cloth or tea towel. A bag of frozen vegetables makes a good ice pack. It's recommended that you wear flat or low-heeled, wide-fitting shoes if you have a bunion. Shoes made from soft leather are ideal because they'll relieve any pressure on the bunion. Avoid narrow or slip-on shoes. High heels can also make your bunion worse by putting excessive pressure on your toes.  Surgical Treatment If the conservative options fail, your doctor will determine the best surgical procedure based on the severity of your condition. The most common surgical procedure is a bunionectomy, which includes removing swollen tissue from around your big toe joint. Removing part of the bone to straighten your big toe. Realigning the metatarsal bone to reduce angular deformity. Joining the bones in a corrected position to permanently correct the deformity. Most people can get up and walk around the day after bunion surgery, but full recovery can occasionally take up to eight weeks or more. Doctors stress the importance of wearing proper shoes, especially after treatment, to prevent recurrence. If you are at higher risk or prone to bunions, you may not be able to avoid recurrence. Prevention To help prevent bunions be sure your shoes don't cramp or irritate your toes. Choose shoes with a wide toe box - there should be space between the tip of your longest toe and the end of the shoe. Your shoes should conform to the shape of your feet without squeezing or pressing any part of your foot. Avoid pointy-toed shoes. Overview
Over-pronation is very common and affects millions of Australians. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% have a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite, a high arched foot. Most of us have a low arch. The foot actually appears quite normal and a clear (but low) arch is present under the foot, especially when sitting down. The situation changes with weight-bearing: when we get up the arch lowers. When we start walking the arches collapse and the ankles roll inwards. This is called over-pronation or fallen arches. Over-pronation is not the same as flat feet as often noted.  Causes There is a relationship between biomechanics and injury that is specific to each body part. Overall though, poor mechanics will either increase the landing forces acting on the body or increase the work to be done by the muscles. Both increase the stress, which, depending on the individual and the amount of running can become excessive and cause injury. Symptoms If you overpronate, your symptoms may include discomfort in the arch and sole of foot, your foot may appear to turn outward at the ankle, your shoes wear down faster on the medial (inner) side of your shoes. Pain in ankle, shins, knees, or hips, especially when walking or running are classic symptoms of overpronation. Overpronation can lead to additional problems with your feet, ankles, and knees. Runners in particular find that overpronation can lead to shin splints, tarsal tunnel syndrome, plantar fasciitis, compartment syndrome, achilles tendonitis, bunions or hallux valgus, patello-femoral pain syndrome, heel spurs, metatarsalgia. Diagnosis Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.  Non Surgical Treatment Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improper fitting footwear can lead to additional problems of the foot. Surgical Treatment Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision. Overview
Sever's Disease is not a disease in the sense of an infection or other chronic pathology but is an injury/irritation of a growth plate. The Calcaneal growth plate or growth plate in the heel bone has attachments from the achilles tendon and the plantar fascia. Pull from either or both of these structures can cause enough motion within the apophysis or growth plate space to create irritation and inflammation which can be quite painful and limiting. This can start when the growth plate is still wide open but is more often seen as the growth plate starts to close further limiting its ability to move with the traction of soft tissue attachments. It was believed by Sever that fractures within the growth plate were the source of the discomfort. When looking at a growth plate that has started to close it can appear to be fragmented into 2 or 3 pieces. It has since been proven that this is the normal appearance of a closing growth plate. Causes Sever disease, like other similar conditions (eg, Osgood-Schlatter disease, little-leaguer's elbow, and iliac apophysitis), is believed to be caused by decreased resistance to shear stress at the bone-growth plate interface. Studies have indicated that traction apophyses have a higher composition of fibrocartilage than epiphyses subjected more to axial load, which are composed predominantly of hyaline cartilage. The anatomy of the calcaneal apophysis lends to significant shear stress because of its vertical orientation and the direction of pull from the strong gastrocnemius-soleus muscle group. Symptoms Sever?s is recognized by pain in the back and lower regions of the heel. It usually starts during or immediately following the child's growth spurt, and/or in very active individuals. The child will usually have pain during or following participation in sport, and will often be seen limping off the field or court. Symptoms of Sever's include painful heel, no swelling or warmth, night pain is absent, pain is worse with increased activity, pain which is usually relieved by rest. Children often hobble or limp from the sports field. Diagnosis The x-ray appearance usually shows the apophysis to be divided into multiple parts. Sometimes a series of small fragments is noted. Asymptomatic heels may also show x-ray findings of resporption, fragmentation and increased density. But they occur much less often in the normal foot. Pulling or ?traction? of the Achilles tendon on the unossified growth plate is a likely contributing factor to Sever?s disease. Excessive pronation and a tight Achilles and limited dorsiflexion may also contribute to the development of this condition. Non Surgical Treatment * Cold packs: Apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking. * Shoe inserts: Small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term. * Medication: Pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor). * Anti-inflammatory creams: Also an effective management tool. * Splinting or casting: In severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare. * Time: Generally the pain will ease in one to two weeks, although there may be flare-ups from time to time. * Correction of any biomechanical issues: A physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition. * Education: Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Overview
 Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus. Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus.Causes The cause of Achilles tendon ruptures besides obviously direct trauma, is multifactorial. In many instances the rupture occurs about 2-6 cm before its attachment to the calcaneous (heel bone). In this area there is a weaker blood supply making it more susceptible to injury and rupture. Rigid soled shoes can also be the causative factor in combination with the structure of your foot being susceptible to injury. Symptoms Many people say that a ruptured Achilles feels like ?being shot in the heel?, if you can imagine how enjoyable that feels. You may hear a snap sound or feel a sudden sharp pain when the tendon tears. After a few moments, the pain settles and the back of the lower leg aches. You can walk and bear weight, but you may find it difficult to point the foot downward or push off the ground on the affected side. You will be unable to stand on tiptoe. Bruising and swelling are likely, and persistent pain will be present. Similar symptoms may be caused by an inflamed Achilles tendon (Achilles tendonitis), a torn calf muscle, arthritis of the ankle, or deep vein thrombosis in the calf, so an MRI or ultrasound scan will likely be used to diagnose your condition. Diagnosis During the clinical examination, the patient will have significantly reduced ankle plantar flexion strength on the involved side. When the tendon is palpated with one finger on either side, the tendon can be followed from the calcaneus to where it "disappears" in the area of the rupture and to where it then returns 2 to 3 cm proximal to the rupture. If the injury is recent, the patient indicates that her pain is localized at the site of the rupture. The defect eventually fills with blood and edema and the skin over the area becomes ecchymotic. Non Surgical Treatment The most widely used method of non-surgical treatment involves the use of serial casting with gradual progression from plantar flexion to neutral or using a solid removable boot with heel inserts to bring the ends of the tendon closer together. The advantage of a solid removable boot is that it allows the patient to begin early motion and is removable. Wide variability exists among surgeons in regards to the period of absolute immobilization, initiating range of motion exercises, and progression of weight bearing status.  Surgical Treatment Surgical repair is a common method of treatment of acute Achilles rupture in North America because, despite a higher risk of overall complications, it has been believed to offer a reduced risk of rerupture. However, more recent trials, particularly those using functional bracing with early range of motion, have challenged this belief. The aim of this meta-analysis was to compare surgical treatment and conservative treatment with regard to the rerupture rate, the overall rate of other complications, return to work, calf circumference, and functional outcomes, as well as to examine the effects of early range of motion on the rerupture rate. Overview
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.  Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities. Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment The key to treatment of LLD in a child is to predict what the discrepancy is at maturity. If it is predicted to be less than 2 cm., no treatment is needed. Limb length discrepancies of up to 2 or 2.5 cm. can be compensated very well with a lift in the shoe. Beyond 2.5 cm., it becomes increasingly difficult to compensate with a left in the insole. Building up the shoe becomes uncosmetic and cumbersome, and some other way of compensating for the discrepancy becomes necessary. The treatment of LLD is long-term treatment, and involves the physician and patient?s family working together as a team. The family needs to weigh the various options available. If leg lengthening is decided on, the family needs to understand the commitment necessary to see it through. The treatment takes 6 months to a year for completion, and complications can happen. But when it works, the results are gratifying.  Surgical Treatment Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Overview
The posterior tibialis muscle originates on the bones of the leg (tibia and fibula). This muscle then passes behind the medial (inside) aspect of the ankle and attaches to the medial midfoot as the posterior tibial tendon. The posterior tibial tendon serves to invert (roll inward) the foot and maintain the arch of the foot. This tendon plays a central role in maintaining the normal alignment of the foot and also in enabling normal gait (walking). In addition to tendons running across the ankle and foot joints, a number of ligaments span and stabilize these joints. The ligaments at the medial ankle can become stretched and contribute to the progressive flattening of the arch. Several muscles and tendons around the ankle and foot act to counter-balance the action of the posterior tibial tendon. Under normal circumstances, the result is a balanced ankle and foot with normal motion. When the posterior tibial tendon fails, the other muscles and tendons become relatively over-powering. These muscles then contribute to the progressive deformity seen with this disorder.  Causes Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder. Symptoms The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels. Diagnosis In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot. Non surgical Treatment Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.  Surgical Treatment A new type of surgery has been developed in which surgeons can re-construct the flat foot deformity and also the deltoid ligament using a tendon called the peroneus longus. A person is able to function fully without use of the peroneus longus but they can also be taken from deceased donors if needed. The new surgery was performed on four men and one woman. An improved alignment of the ankle was still evident nine years later, and all had good mobility 8 to 10 years after the surgery. None had developed arthritis.
Overview
When we have foot pain, it isn?t always easy to pinpoint the source because we can?t visualize the structure of all the bones, muscles, and tendons on the inside. The posterior tibial tendon plays an important supportive role within the structure of the foot. It attaches to your calf muscle and then comes down along the inside of your ankle, connecting to the bones inside your foot at the other side. This tendon?s main function is to hold up your arch and support your foot during each and every movement. Every step, run, walk, or jump is made possible with the support from this crucial tendon. While it is designed to perform such an important role, it is vulnerable to stress and injury. A tear during a traumatic injury or stress from overuse can injure the tissues within the tendon. This kind of injury is referred to as posterior tibial tendon dysfunction (PTTD). A really hard fall during a sports game or exposure to a repetitive motion, such as the impact on feet during soccer, tennis, football or basketball, can cause an injury. Flat foot and flat feet in adults can exacerbate this condition. The tendon can experience small tears and become inflamed. If the inflammation is allowed to continue and worsen over time, it will weaken further and could rupture completely.  Causes Rheumatoid arthritis This type of arthritis attacks the cartilage in the foot, leading to pain and flat feet. It is caused by auto-immune disease, where the body?s immune system attacks its own tissues. Diabetes. Having diabetes can cause nerve damage and affect the feeling in your feet and cause arch collapse. Bones can also fracture but some patients may not feel any pain due to the nerve damage. Obesity and/or hypertension (high blood pressure) This increases your risk of tendon damage and resulting flat foot. Symptoms Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot. Diagnosis There are four stages of adult-acquired flatfoot deformity (AAFD). The severity of the deformity determines your stage. For example, Stage I means there is a flatfoot position but without deformity. Pain and swelling from tendinitis is common in this stage. Stage II there is a change in the foot alignment. This means a deformity is starting to develop. The physician can still move the bones back into place manually (passively). Stage III adult-acquired flatfoot deformity (AAFD) tells us there is a fixed deformity. This means the ankle is stiff or rigid and doesn???t move beyond a neutral (midline) position. Stage IV is characterized by deformity in the foot and the ankle. The deformity may be flexible or fixed. The joints often show signs of degenerative joint disease (arthritis). Non surgical Treatment Icing and anti-inflammatory medications can reduce inflammation and physical therapy can strengthen the tibial tendon. Orthotic inserts that go inside your shoes are a common way to treat and prevent flatfoot pain. Orthotics control the position of the foot and alleviate areas of pressure. In some cases immobilization in a cast or walking boot is necessary to relieve symptoms, and in severe cases surgery may be required to repair tendon damage. 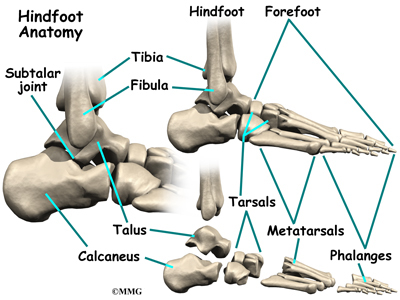 Surgical Treatment Good to excellent results for more than 80% of patients have been reported at five years' follow up for the surgical interventions recommended below. However, the postoperative recovery is a lengthy process, and most surgical procedures require patients to wear a plaster cast for two to three months. Although many patients report that their function is well improved by six months, in our experience a year is required to recover truly and gain full functional improvement after the surgery. Clearly, some patients are not candidates for such major reconstructive surgery. |
